Case History:
- A 45 year old chronic alcoholic and smoker comes to your clinic with complaints of throat irritation and cough especially at night for 4 months duration. The irritation is there in the morning but goes out as the day progresses. He has no other complaints except for occasional water brash. His vitals are normal and physical examintaion reveals throat congestion. Rest of the examination is normal. How will you reach the diagnosis and manage this case?
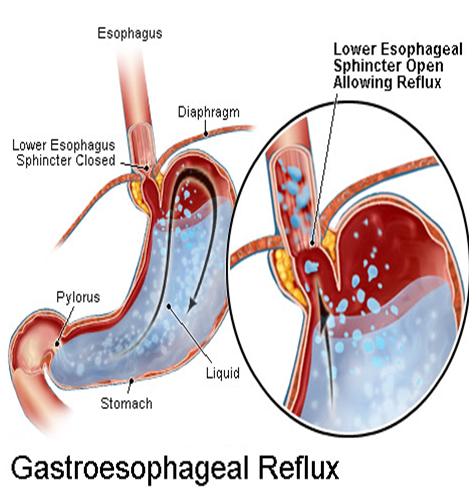
Gastroesophageal Reflux Disease(GERD)
Objectives
- Definition
- Classification
- Epidemiology
- Etiology and Pathogenesis
- Clinical Manisfestations
- Diagnosis
- Differential diagnosis
- Treatment
GERD is defined as chronic symptoms or mucosa damage produced by the abnormal reflux in the esophagus
Heartburn, water brash
superficial linear ulcer, erosion,redness,friability,bleeding,exudate,erythema,engorgement
2. Classification
(1) Non-erosive esophagitis (NERD)
(2) Erosive esophagitis(EE) or reflux
esophagitis(RE)
(3) Barrett’s esophagus (BE)
(1) Non-erosive esophagitis (NERD):
- the presence of typical symptoms of GERD caused by intra-esophageal acid
- the absence of visible esophageal mucosa injury at endoscopes
(2) Erosive esophagitis(EE) or reflux esophagitis(RE) :
- the presence of typical symptoms visible esophageal mucosa injury at endoscopes
.png)
(3)Barrett’s Esophagus (BE)
- Acid damages lining of esophagus and causes chronic esophagitis
- Damaged area heals in a metaplastic process and abnormal columnar cells replace squamous cells
.png)
- This specialized intestinal metaplasia(IM) can progress to dysplasia and adenocarcinoma
- Many patients with Barrett’s are asymptomatic
3. Epidemiology
- GERD is one of the most prevalent gastrointestinal disorders
- GERD increases by age, the peak prevalence is in those people whose age is between 40-60ys.There is no difference between male and female
- GERD in Asian population is not as usual in the Americans
(1) Genetic factors
(2) Low maximal acid output/small parietal cell mass
(3) High LES(lower esophagus sphincter) pressure
(4) Low BMI (body mass index)
(5) Lower consumption of alcohol, coffee, tea
(6) Lower or Less Smoking
(7) Fewer aggravating medicines
(8) Dietary factors(Lower dietary fat and chocolate in asian food)
(9) Lower consumption of carbonated soft drinks
(10)Lower consumption of citric fruit drinks

(1)Defense barrier against reflux consists of
- tonic activity of the LES supported by crural diaphragm.
- The ana’tomical location of the gastroesophageal junction below the diaphragmatic hiatus
- Among them, the LES is primary barrier to gastroesophageal reflux , its basal pressure is 10-30mmHg
- LES normally works in conjunction with the diaphragm

- If barriers disrupted, gastric contents go from stomach to esophagus.
- In other words,reflux occurs only when the gradient of pressure between the LES and the stomach is lost.
- The gradient of pressure lost can be caused by a sustained or transient decrease in LES tone
A sustained hypotension of the LES (Defective basal LES pressure)may be due to :
- muscle weaknes that is without apparent cause
- scleroderma-like disease, myopathy associated with chronic intestinal pseudo-obstruction, pregnancy, smoking, anticholinergic drugs, smooth-muscle relaxants[β-adrenergic drugs, aminophylline, nitrates, calcium channel blockers, phosphodiesterase inhibitors that increase cyclic AMP or cyclic GMP(including sildenafil), surgical damage to the LES, and esophagitis
- Defective LES: transient LES relaxation (TLESR)increase frequency of reflux
- TLESR without associated esophageal contraction is due to vagal reflex in which LES relaxation is elicited by gastric distention
- Increased episodes of TLESR are associated with GERD.
- A similar reflex operates during belching.
- when gastric volume is increased (after meal, in pyloric obstruction, in gastric stasis, during acid hypersecretion states)
- when gastric contents are near the gastroesophageal junction(in recumbency, bending down, hiatus hernia)
- when gastric pressure is increased (obesity, pregnancy, ascites, tight clothes)
- It means that esophageal peristaltic contraction may clear materials refluxed to esophagus in normal condition
- When Peristaltic contraction is impaired, Esophageal clearance is impaired
- It includes esophageal mucous epithelium and good blood circulation in submucous layer
- Some factors ( e.g, smoking, alcohol, depression ) may injury this barrier and lead to RE.
- Exposure depends on the amount of refluxed material per episode, frequency of episodes, and rate of clearing the esophagus by gravity and peristaltic contractions
- Acid refluxed into the esophagus is neutralized by saliva. Thus, impaired salivary secretion also increases esophageal exposure time
- If the refluxed material extends to the cervical esophagus and breaches the upper sphincter , it can enter the pharynx, larynx and trachea
5. Clinical Manisfestations

(1)Esophageal symptoms --Most common symptoms
Heartburn—retrosternal burning discomfort
Regurgitation—effortless return of gastric contents into the pharynx without nausea, retching, or abdominal contractions
Dysphagia—difficulty(or trouble )swallowing
Chest pain
(1)Esophageal symptoms -- Less common symptoms
- pain with swallowing (odynophagia)
- nausea
(2) Extraesophageal symptoms
Asthma, laryngitis, chronic cough, earache, gingivitis, eroded tooth enamel, globus sensation, hoarseness, sore throat
(3) complications
- Erosive esophagitis
- Peptic stricture
- Barrett’s esophagus
6. Diagnosis
- If classic symptoms of heartburn and regurgitation exist in the absence of “alarm symptoms”, the diagnosis of GERD can be made clinically and treatment can be initiated
(1) When to investigate?
Investigations are warranted if,
a) the diagnosis is unclear
b) symptoms persist or are refractory to treatment
c) complications suspected with presence of alarm symptoms
※Alarm symptoms:
- BW loss > 10%
- Persistent vomiting
- Anemia, bleeding (Hematemesis, Melena)
- Progressive dysphagia or odynophagia
- Family UGI (upper gastrointestinal) cancer
(2) Which investigation?
a) Barium swallow and meal: may be useful in: persistent dysphagia caused by suspected stricture or the assessment of large hiatus hernia
b) Endoscopes[highly specific (90-95%)] :
(i) Most sensitive test for reflux esophagitis, diagnosis of other mucosal lesions
(ii) Only sensitive method for diagnosing Barrette’s esophagus
(iii) Recognition and management of peptic stricture
Trial of Medications
- H2 blockers (H2 receptor blocking agents) or PPI (proton pump inhibitors)
- Expect response in 2-4 weeks
- If no response
- Change from H2RA to PPI
- Maximize dose of PPI

If PPI response inadequate despite maximal dosage
- Confirm diagnosis
- EGD (Esophagogastrodudenoscopy)
- 24 hour pH monitoring
Esophagogastrodudenoscopy (EGD)
.png)
Endoscopy (with biopsy if needed)
Patients who need EGD
- Alarm symptoms
- Poor therapeutic response
- Long symptom duration
- Lacks sensitivity for identifying pathologic reflux
- Absence of endoscopic features does not exclude a GERD diagnosis

7.Differential diagnosis
- Symptoms of GERD may be similar to those of other diseases such as esophageal motility disorders, peptic ulcer,cholelithiasis, nonulcer dyspepsia, and angina pectoris
- Furthermore, RE may be confused with pill-induced damage, radiation esophagitis ,or infections (cytomegalo’virus, herpes, Candida)
8. Treatment
Goals of therapy
- Symptomatic relief
- Heal esophagitis
- Avoid complications
Current Management for GERD
(1) Life-style modification
(2) Medical therapy
(4) Surgery
(5) Management of Complications
(1) Lifestyle modifications
- Avoid large meals (Avoid over food)
- Avoid acidic foods (citrus/tomato), alcohol, caffiene, chocolate, onions, garlic, peppermint
- Decrease fat intake
- Avoid lying down within 3-4 hours after a meal
- Elevate head of bed 4-8 inches – very effective
- Avoid meds that may potentiate GERD (CCB, alpha agonists, theophylline, nitrates, sedatives, NSAIDS)
- Avoid clothing that is tight around the waist
- Lose weight
- Stop smoking
(2) Medical therapy for GERD
- Antacids
- Proton Pump Inhibitors(PPI)
- H2 blockers
- Prokinetic agents: Cisapride, Metoclopramide, Erythromycin
(4) Antireflux surgery
- Antireflux surgery( indications)
- Failed medical management
- Patient preference
- GERD complications
- Medical complications attributable to a large hiatal hernia
- Atypical symptoms with reflux documented on 24-hour pH monitoring
(5) Management of Complications
Barrett’s Esophagus
- Manage in same manner as GERD
- EGD every 3 years in patients without dysplasia
- In patients with dysplasia annual to shorter interval surveillance
(5) Management of Complications
- Esophageal stricture
- May need dilation
